Abstract
Background
Fibre is promoted as part of a healthy dietary pattern and in diabetes management. We have considered the role of high-fibre diets on mortality and increasing fibre intake on glycaemic control and other cardiometabolic risk factors of adults with prediabetes or diabetes.
Methods and findings
We conducted a systematic review of published literature to identify prospective studies or controlled trials that have examined the effects of a higher fibre intake without additional dietary or other lifestyle modification in adults with prediabetes, gestational diabetes, type 1 diabetes, and type 2 diabetes. Meta-analyses were undertaken to determine the effects of higher fibre intake on all-cause and cardiovascular mortality and increasing fibre intake on glycaemic control and a range of cardiometabolic risk factors. For trials, meta regression analyses identified further variables that influenced the pooled findings. Dose response testing was undertaken; Grading of Recommendations Assessment, Development and Evaluation (GRADE) protocols were followed to assess the quality of evidence. Two multicountry cohorts of 8,300 adults with type 1 or type 2 diabetes followed on average for 8.8 years and 42 trials including 1,789 adults with prediabetes, type 1, or type 2 diabetes were identified. Prospective cohort data indicate an absolute reduction of 14 fewer deaths (95% confidence interval (CI) 4–19) per 1,000 participants over the study duration, when comparing a daily dietary fibre intake of 35 g with the average intake of 19 g, with a clear dose response relationship apparent. Increased fibre intakes reduced glycated haemoglobin (HbA1c; mean difference [MD] −2.00 mmol/mol, 95% CI −3.30 to −0.71 from 33 trials), fasting plasma glucose (MD −0.56 mmol/L, 95% CI −0.73 to −0.38 from 34 trials), insulin (standardised mean difference [SMD] −2.03, 95% CI −2.92 to −1.13 from 19 trials), homeostatic model assessment of insulin resistance (HOMA IR; MD −1.24 mg/dL, 95% CI −1.72 to −0.76 from 9 trials), total cholesterol (MD −0.34 mmol/L, 95% CI −0.46 to −0.22 from 27 trials), low-density lipoprotein (LDL) cholesterol (MD −0.17 mmol/L, 95% CI −0.27 to −0.08 from 21 trials), triglycerides (MD −0.16 mmol/L, 95% CI −0.23 to −0.09 from 28 trials), body weight (MD −0.56 kg, 95% CI −0.98 to −0.13 from 18 trials), Body Mass Index (BMI; MD −0.36, 95% CI −0·55 to −0·16 from 14 trials), and C-reactive protein (SMD −2.80, 95% CI −4.52 to −1.09 from 7 trials) when compared with lower fibre diets. All trial analyses were subject to high heterogeneity. Key variables beyond increasing fibre intake were the fibre intake at baseline, the global region where the trials were conducted, and participant inclusion criteria other than diabetes type. Potential limitations were the lack of prospective cohort data in non-European countries and the lack of long-term (12 months or greater) controlled trials of increasing fibre intakes in adults with diabetes.
Conclusions
Higher-fibre diets are an important component of diabetes management, resulting in improvements in measures of glycaemic control, blood lipids, body weight, and inflammation, as well as a reduction in premature mortality. These benefits were not confined to any fibre type or to any type of diabetes and were apparent across the range of intakes, although greater improvements in glycaemic control were observed for those moving from low to moderate or high intakes. Based on these findings, increasing daily fibre intake by 15 g or to 35 g might be a reasonable target that would be expected to reduce risk of premature mortality in adults with diabetes.
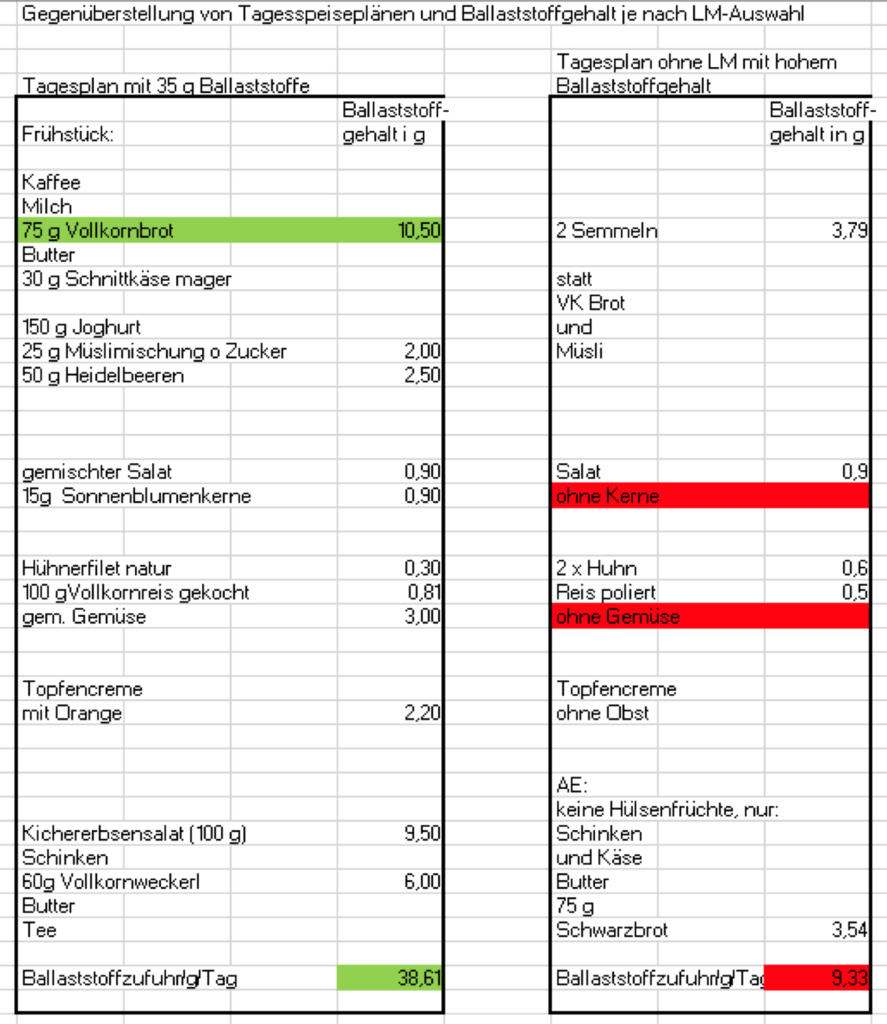
Fazit:
Wir sollten in der Praxis kurze Incentives setzen, die den Patienten helfen, in ihrem gewohnten täglichen Leben Ernährung ohne großen Aufwand zu modifizieren. Ballaststoffe sind hier eine wichtige Hilfe. Dafür sollten wir gute Beispiele haben und weitergeben.
Fazit:
Haferflockentage in der Woche einrichten. Und kleine Veränderungen im gewohnten täglichen Leben initiieren.