Abstract: Pulmonary embolism has extremely varied clinical presentations and can be difficult to diagnose. Clinical decision rules can help determine the probability of pulmonary embolism by assessment of the clinical presentation. After the diagnosis,several prognostic rules can be used to risk-stratify and facilitate outpatient treatment of pulmonary embolism. This review addresses the utility of clinical decision rules, biomarkers in the diagnosis of pulmonary embolism, high-risk patient phenotypes, the use of this data to make disposition decisions for patients with a diagnosis of PE, and recent shifts in the management of pulmonary embolism in the clinical setting.
Full Text für die Interessierten: https://sci-hub.st/10.1016/j.jen.2020.02.018
Zusammenfassung:
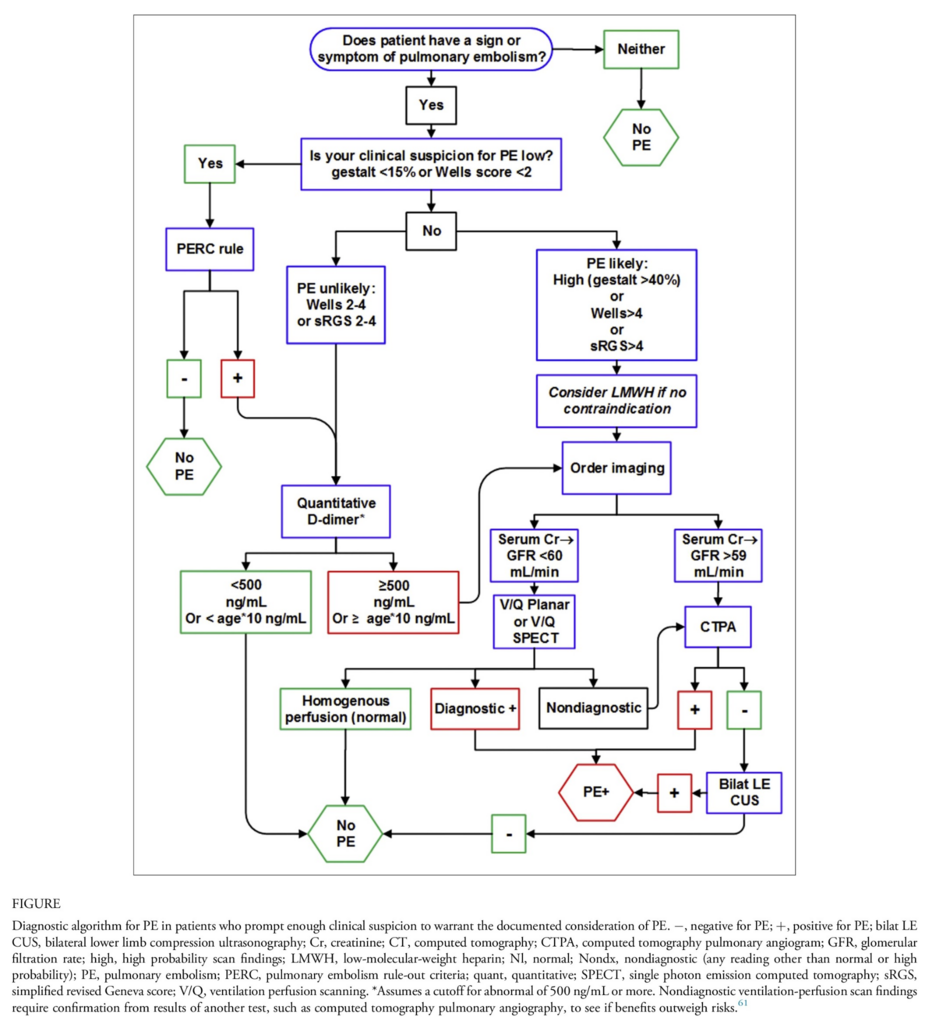
– bei einem WELLS-Score von 0 oder 1 machen wir den PERC, wenn dieser bei 0 liegt gilt die LAE als ausgeschlossen (Wahrscheinlichkeit <2%, siehe https://sci-hub.st/10.1111/j.1538-7836.2008.02944.x)
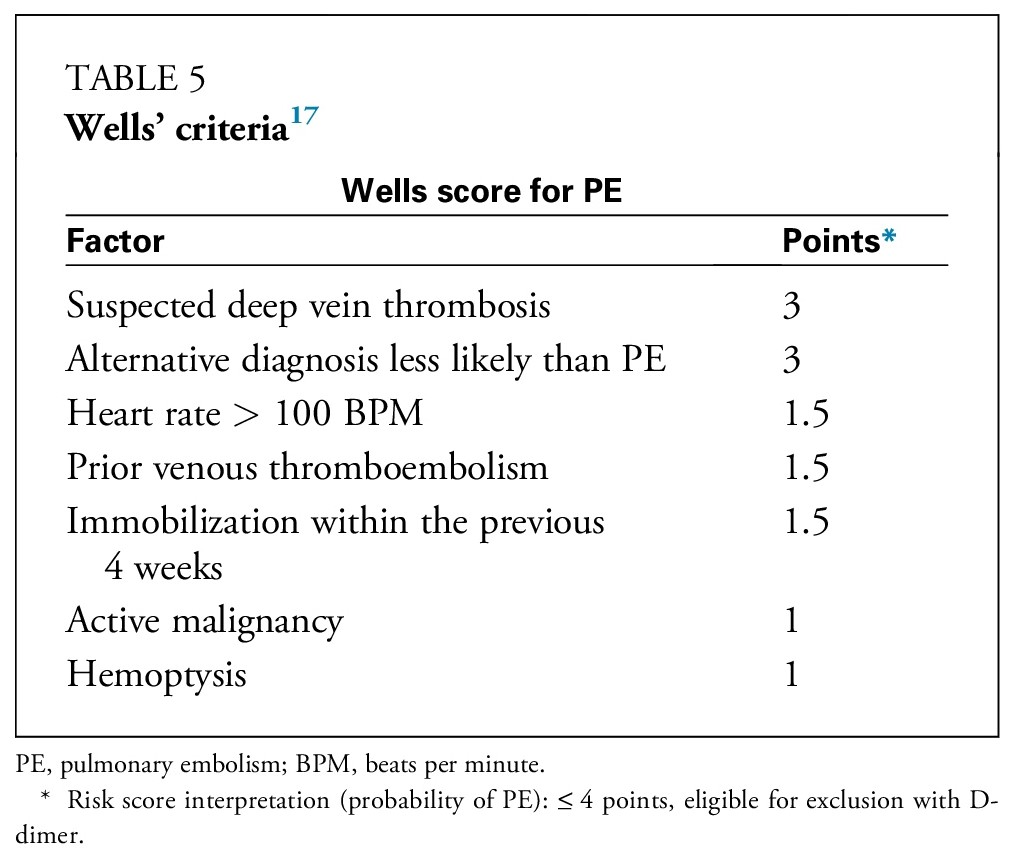
– bei einem WELLS-Score von 2,3 oder 4 entscheidet der D-Dimer-Test und
– bei einem WELLS-Score von 5 ode höher braucht es eh die Bildgebung.
Kennt ihr diesen Score? Verwenden wir ihn aus einem bestimmten Grund nicht in der Praxis? Ich hatte noch nie von ihm gehört und finde ihn sehr praktisch im ZNA-Kontext.
Fazit:
PERC-Score kann gerade bei jungen Frauen ohne Kontrazeptiva mit Atemnot und Sorgen eine Hilfe darstellen. Zusätzlich zum Wells-Score.
Fazit Regen:
PERC-Score kann eine wichtige Ergänzung in der Vermeidung von unnötiger weiterer Diagnostik sein und abwendbar gefährliche Verläufe ausschließen.